

Introduction
AML primarily affects older adults and long-term survival in this group is poor. Despite data showing improvement in outcomes of adults aged<80 with utilization of intensive induction chemotherapy and allogeneic HSCT, these are underutilized. In this study, we report our center experience, focusing on HSCT referral and utilization rates in older adults, as well as the reasons for non-referral and utilization.
Methods
We performed a retrospective analysis of consecutive patients aged ≥60 evaluated at an academic cancer center between Jan 2014 and Dec 2017. We included patients who were diagnosed and received all treatment at our center (N=101), as well as patients referred from outside institutions for HSCT who did not receive initial treatment at our center (N=12). We collected demographics, disease and treatment characteristics, responses, and outcomes. For patients diagnosed and treated at our center, we determined whether discussion about HSCT was documented, rates of HSCT referral and utilization, and time from diagnosis to HSCT referral and utilization. For patients who were referred for HSCT only, we determined HSCT rates and time from diagnosis to HSCT. Fisher's exact test was used to assess the association of patient factors with HSCT referral and utilization. A Cox model was used to assess the association of HSCT (via a time-dependent covariate) with relapse-free survival (RFS) and overall survival (OS).
Results
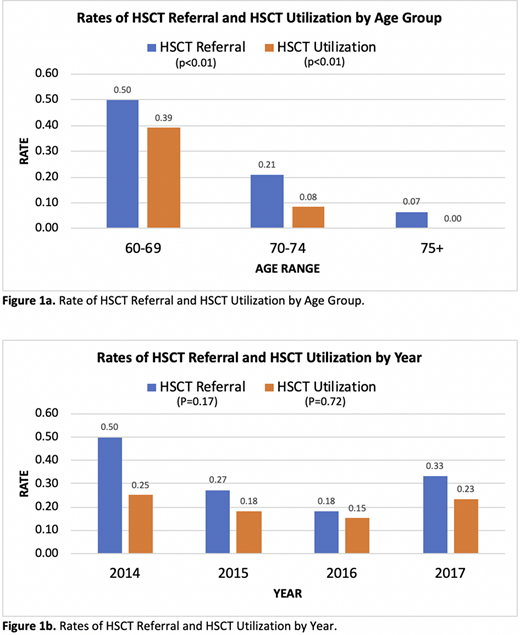
Median age was 70 years (IQR 10), 53% were male, and 91% were white. Among patients who were diagnosed and received all treatment at our center, 30% (N=30/101) were referred for HSCT, and 20% (20/101) received HSCT. Among patients who were referred from outside institutions, 42% (N=5/12) received HSCT. Thirty-seven percent (N=37/101) had a documented discussion regarding HSCT and referral was made for 81% (N=30/37). Common documented reasons (can be multiple) for not referring a patient were: performance status (N=20), advanced age (N=15), patient refusal (N=13), refractory disease (N=11), and prohibitive comorbidity (N=6). Reasons were not documented in 22 patients. Among the patients who were referred but did not receive HSCT (N=10/30), common documented reasons for not proceeding with HSCT were: refractory disease (N=5), advanced age (N=2), and prohibitive comorbidity (N=1). HSCT referral and utilization rates decreased with increasing age (Figure 1a) and were similar from 2014-2017 (Figure 1b). Patients referred for HSCT were more likely to be younger (median 66.0 vs 73.0 years, p<0.01), had fewer comorbidities (1.0 vs. 2.0, p=0.02), normal cytogenetics (53 vs. 31%, p=0.04), received intensive chemotherapy (83 vs. 39%, p<0.01), and achieved complete response (CR) or CR with incomplete count recovery (CRi; 80 vs. 30%, p<0.01) prior to HSCT. Patients who received HSCT had similar characteristics. Time to HSCT referral did not differ between patients diagnosed and treated our center vs. those referred from outside institutions [2.8 vs. 2.3 months (mo), p=0.74]. Time from diagnosis to HSCT also did not differ between the two groups (5.1 vs. 7.1 mo, p=0.57). With a median follow-up of 40 mo, median OS from time of diagnosis was 12.1 mo [95% Confidence Interval (CI): 8.7-16.8 mo] in the whole sample. In the HSCT group, median RFS was 16.4 mo and median OS was 30.0 mo from time of HSCT. On Cox regression model, there was insufficient evidence for association of transplant with survival in this patient population (p=0.18), after adjusting for age. Age was associated with worse OS (HR 1.06, 95% CI 1.03-1.09).
Conclusions
Our study highlights that HSCT referral and utilization rates for older adults with AML are low and have not increased over time, despite improvement in supportive care, reduced intensity conditioning regimens, and alternate donor sources. Less than half of older patients who received intensive induction therapy were referred for HSCT. We suspect that the increasing use of effective lower intensity therapies will affect these rates as more patients achieve remission without intensive induction. Strategies are needed to improve referral and HSCT rates for older adults, such as formalized fitness assessments, interventions to improve performance status, and more effective therapies to reduce relapse rates. In addition, larger prospective studies are needed to evaluate the utility of HSCT in older adults with AML.
Mendler:Jazz Pharmaceuticals: Speakers Bureau; GLG: Consultancy. Aljitawi:Sanatela Medical: Patents & Royalties: Patent pending. Liesveld:Abbvie: Honoraria; Onconova: Other: data safety monitoring board. Loh:Seattle Genetics: Consultancy; Pfizer: Consultancy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal